Colorectal Conundrum: December 4, 2023
For the Quiz & Answers to last weeks Conundrum - see the blog post here.
Colorectal Conundrum for December 4th:
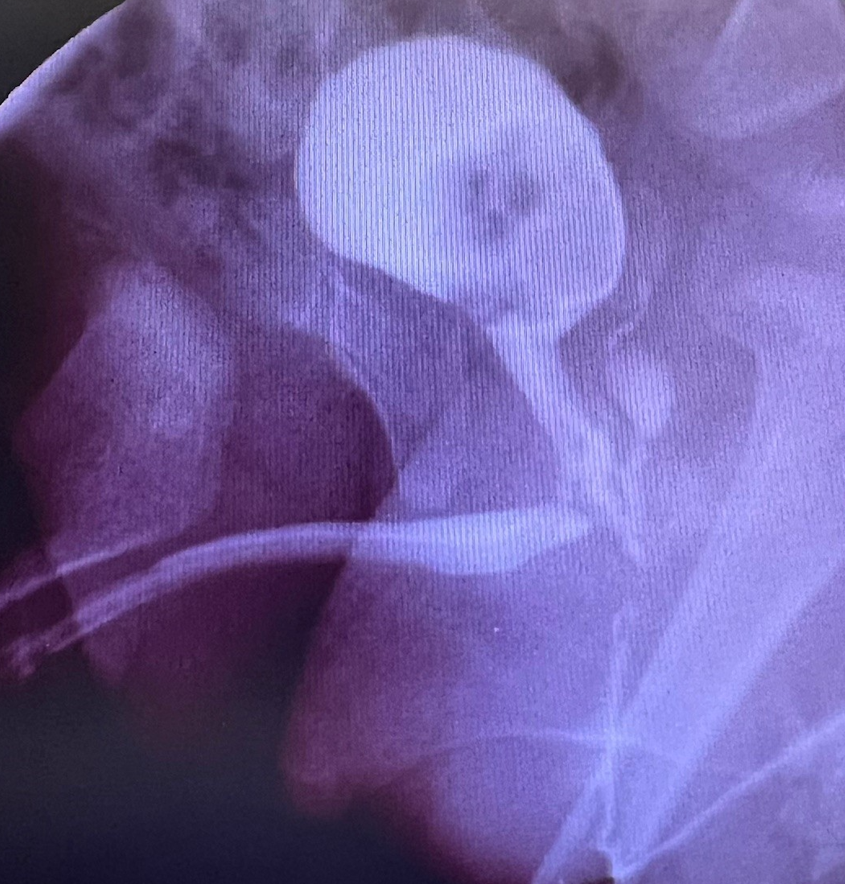
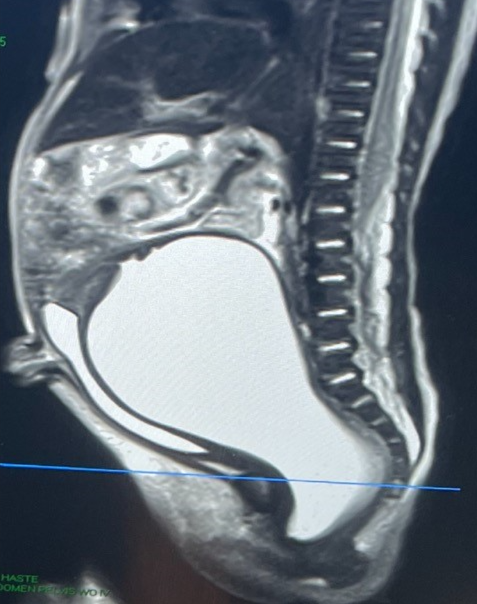
A 9-year-old female with Hirschsprung disease underwent a Yancey-Soave pull-through in the first year of life. She developed constipation and for this was treated with a myectomy. She began to have soiling and also was noted to pass stool via the vagina and for this was diverted with an ileostomy. On your exam her dentate line is absent and her sphincters are patulous, confirmed by anorectal manometry as weak particularly on the left side. She has a rectovaginal fistula and a palpable circumferential cuff. What would you offer this patient.
Answer:
This patient is diverted with an ileostomy, and we need to explain why they needed this diversion – i.e. Is there a distal obstruction? What do we do about the rectovaginal fistula? She has a missing dentate line and patulous sphincters. And a palpable cuff. She needs a redo – repair of the rectovaginal fistula, removal of the cuff, and confirmation that there are good ganglion cells present at the distal pull-through. As for the patulous sphincters – the pull-through can be tacked to the perineal area musculature to perform a sphincter reconstruction.
Here is a useful video of a similar case: https://www.expertsinsurgery.com/programs/sphincter_reconstruction_withlogo-3192d1?category_id=49506
How would you handle this case?