Colorectal Conundrum: December 11, 2023
Colorectal Conundrum for December 11th:
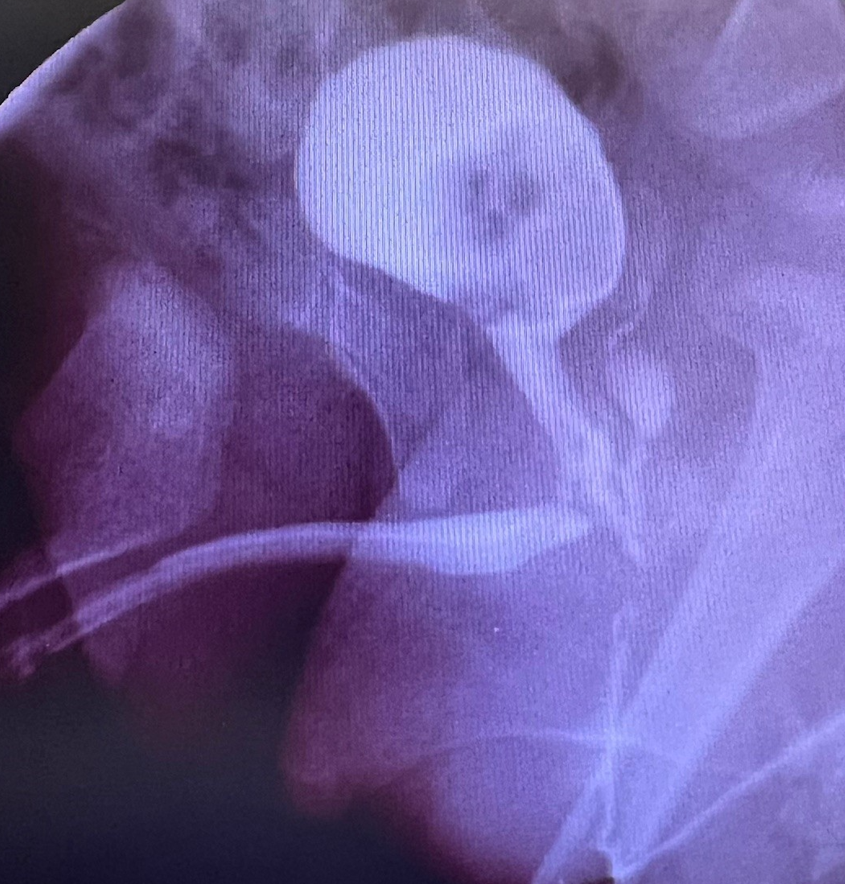
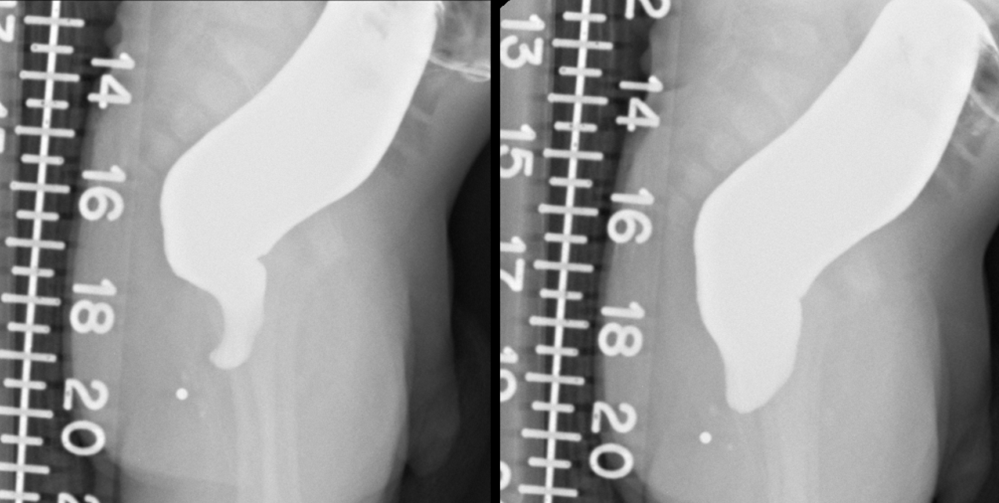
Newborn with normal appearing anus but distended and anal probe didn’t go in more than 1 cm. Surgeons performed an anal exploration, didn’t find a lumen, and then decided to do a colostomy. Below is the distal colostogram.
Questions:
- How do you explain the funny looking presacral space?
- What is the likely diagnosis here?
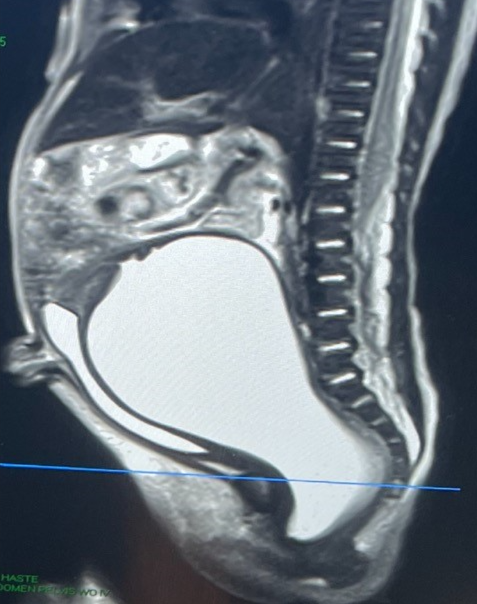
- What work-up is vital to rule out a key associated problem?
Answer:
This is a vitally important type of anorectal malformation to recognize. With a normal anal canal and distal obstruction this could be either anal stenosis or rectal atresia. With no lumen found, this is likely rectal atresia – which led to the colostomy creation. The distal colostogram shows an enlarged presacral space. The flat line on the left image is the levators so that is expected, but even once the distal rectum is distended the presacral bulge persists. All such patients require a pelvic MRI to rule out a presacral mass, and a spinal component to the MRI to be sure there is no dural connection of that mass.
Please see this article: https://pubmed.ncbi.nlm.nih.gov/26902368/
And these videos, found at www.expertsinsurgery.com
How would you handle this case?