Colorectal Conundrum: November 13, 2023
For the Quiz & Answers to last weeks Conundrum - see the blog post here.
Colorectal Conundrum for November 13th:
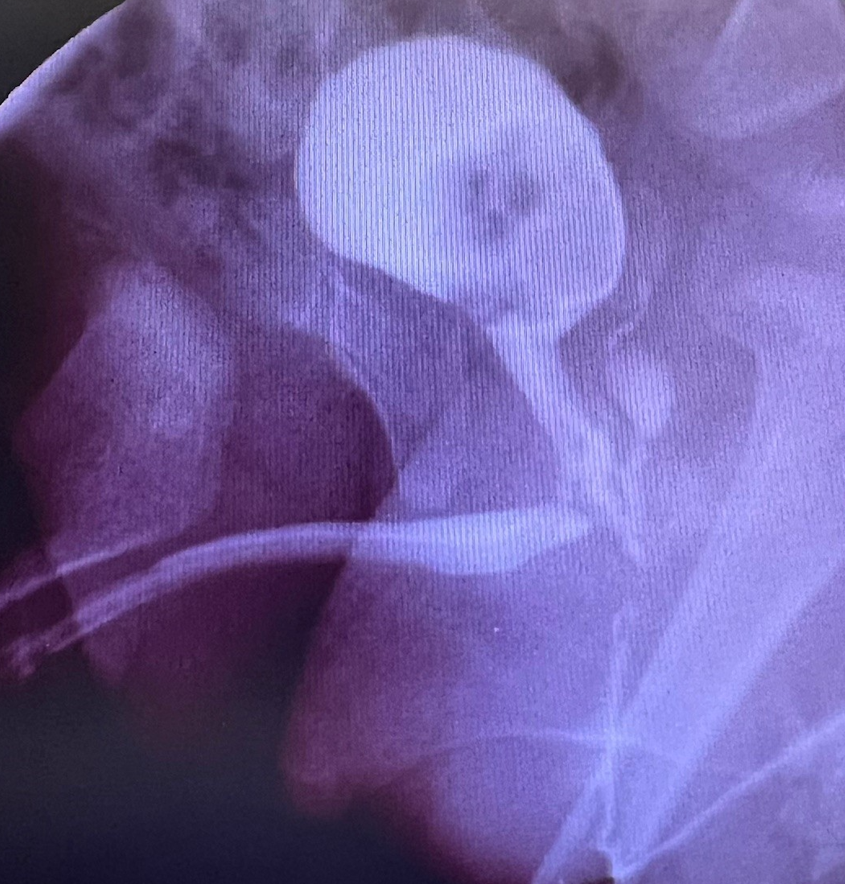
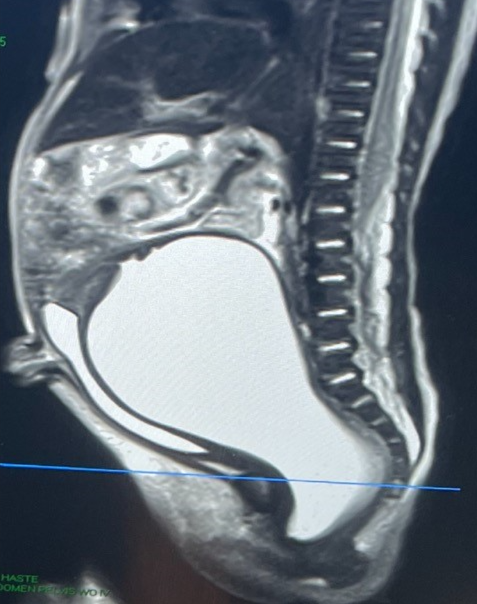
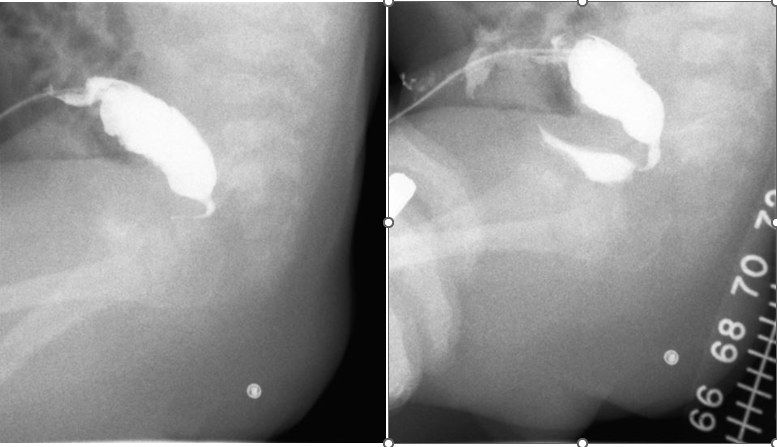
What would you do in this male patient with ARM, newborn colostomy, and now with distal colostogram showing the below finding?
Answer for November 13th: There is much more to this case than meets the eye and several options. The key item to recognize is the very high rectum and short distal piece of bowel given the location of the colostomy. One choice would be to take down the fistula laparoscopically and pull it through, but I caution against leaving a Hartman’s pouch in – the colostomy closure will be super difficult. So one could close the colostomy and then divert above with a more proximal colostomy or with an ileostomy. However, given the potentially poor blood supply of this piece of rectum and to avoid two anastomoses (anoplasty and colo-colonic), plus the new diversion and the stoma closure that goes along with it, and seeing how poor is the sacrum, my choice here would be to pull through the colostomy and remove this distal piece. I know how important is the rectum to provide a reservoir and allow for continence but I am balancing all of that surgery with a likely incontinent child here that would do fine with a sigmoid pulled through and antegrade flushes via the Malone.
How would you handle this case?